
Protecting Progress in Care Delivery
The importance of follow-up, coordination, and managing transitions between settings
Residents leaving a skilled nursing facility (SNF) are encountering a moment of maximum vulnerability when they discharge home. During this especially delicate time, weeks of coordinated, closely managed care give way to a sudden period of independence. What happens in the days and weeks following determines whether the progress during their stay holds or disintegrates.
This article reviews recent research into the risks associated with unmanaged transitions home following hospital and SNF stays, and the association between transitional care management (TCM) programs and improved long-term outcomes.
Transitions are moments of immense risk
A recent study reviewing over 67,000 heart failure hospitalizations discharged to SNFs, then home, found that the first few days after transitioning home carry the highest risk of readmission by a significant factor (Journal of American Medical Directors Association).
Here are the key findings:
- Residents with short stays (1–6 days) had readmission rates 4x higher during the first two days home than the rest of the 30-day window.
- For residents with 1–2 week stays, early risk was more than 2.5x higher.
- Residents with 2–4 week stays had nearly 2x the risk in the first two days home.
The study concludes: “Interventions to improve post-discharge outcomes have primarily focused on hospital discharge. This evidence suggests that interventions to reduce readmissions may be more effective if they also incorporate the SNF-to-home transition.”
Research consistently shows that 12–14% of eligible patients receive TCM following discharge, meaning a vast majority of residents return home from a SNF or acute care stay without true care continuity. (NORC, American Journal of Managed Care).
When you look at national averages, rates may look similar between rehospitalizations from SNFs during a stay and readmissions from home (roughly 20–25%), but the impact on residents—and the impact on the health journey—are very different.
Disruption is more than readmission rates
Once a resident has returned home, they have gone through several weeks of coordinated and closely managed care. Clinical staff put their time, expertise, and hearts into improving a resident’s health, identifying underlying needs, and helping this individual progress to the point they can safely return home (or transition to a long-term care facility).
That vast network of clinical professionals is gone when residents are home.
But the transition is rarely, if ever, a complete, neat move from one state to another. Treatment plans remain fluid, medications are changing, and the entire clinical approach has shifted.
Small changes in a person’s health that might have prompted a discussion can no longer be monitored so closely.
Hospitalizations from home deplete so much of the momentum gathered during their SNF stay and are a major disruption to that individual, not to mention the unquantifiable emotional burden these events incur.
It’s up to administrators and operators to implement data-backed programs that improve outcomes following SNF-to-home discharge
Let’s return to that stat: only 12–14% of residents are leaving facilities with TCM codes. Even within that data point, there’s no guarantee TCM is being implemented most effectively.
Are we checking boxes or delivering real continuity across the change in setting?
20-25% are experiencing readmissions. We don’t need studies to know this is higher when you factor in other social determinants.
Tackling disruption with coordination
At Dartmouth Health, a comprehensive TCM program was implemented across 2,204 patients with results that are replicable for coordinated providers. Readmissions for patients with TCM was 5% compared to 11.9% for those without (Journal of the American Board of Family Medicine).
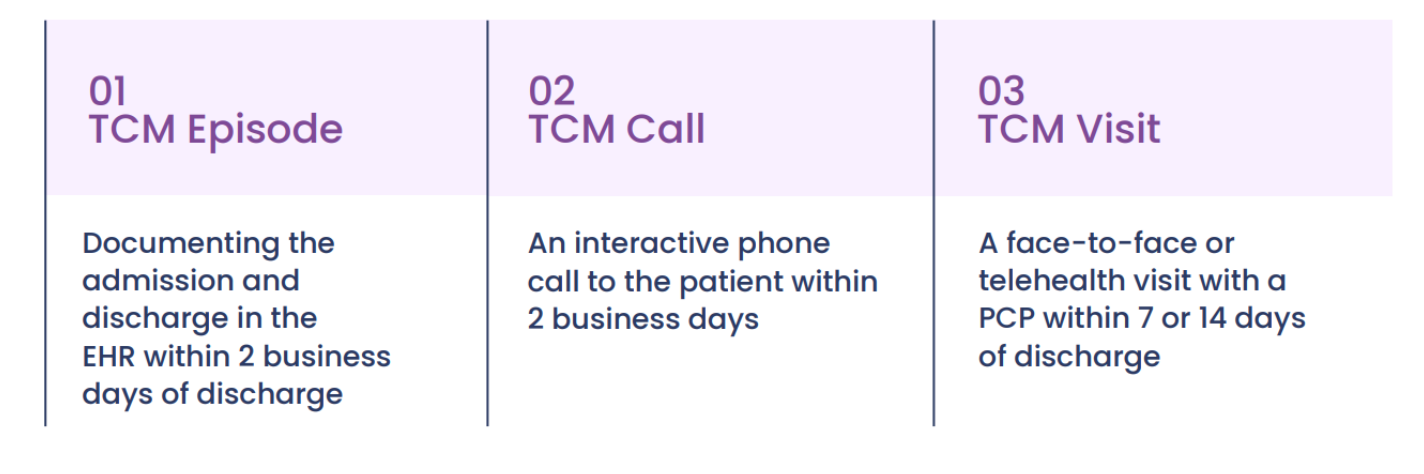
Perhaps most importantly, TCM was only effective when all three elements of the program were implemented. No single component improved outcomes.
Our TCM program at Lumina Care has delivered similar results. From inception to month 5, readmission rates were reduced by 63% for a skilled nursing facility organization with facilities across the northeast.
Continuity and coordination benefit everyone
Administrators and Operators
Over 70% of facilities in CMS’s Value-Based Purchasing Program received a financial penalty in 2024 (around one in three were hit with the maximum rate).
Readmission rates impact Five-Star ratings, which feed directly into referrals, census, and reputation in ways that compound over time. Beginning in FY2025, CMS also added the Discharge to Community measure to the VBP program, making transitions home a scored, public metric.
Investing in a well-managed transition isn’t just the right clinical decision. CMS has made it the right financial one, too, with clear reimbursement pathways that make TCM viable to implement at scale, especially for multi-facility operators. The clinical case and the financial case point in the same direction.
Care Staff
We all want to work in effective care environments. Skilled nursing is no stranger to financial constraints and resource pressure, and research consistently links poor patient outcomes to staff burnout and turnover.
Clinical teams invest significant time and skill in helping residents make tremendous progress. When a resident returns weeks later, it erodes the sense of accomplishment that keeps skilled clinicians in this work.
Residents
A 2025 study published in Medicine found that elderly cardiac patients receiving regular post-discharge follow-up and structured education reported lower anxiety, fewer recurring symptoms, better adherence, and higher treatment satisfaction (Medicine).
While this study population differs from SNF-to-home discharge, the underlying mechanism maps nicely to TCM programs. Keep residents informed, supported, and connected to their care to improve outcomes.
Conclusion: TCM is needed in SNF settings to improve outcomes
Looking at the data, it is clear that TCM programs improve outcomes. For administrators and managing teams, that means better facility performance.
For staff and residents, that means better health outcomes and a proven way to protect the progress made during a SNF stay.
With reimbursement models in place that support TCM, we strongly support the implementation of transitional care management in SNF settings.
This approach is proven to help residents transition home safely, with more clinical support available to help them navigate a complicated home setting while continuing to meet their care needs.