Lumina Care Quarterly:
When care transitions, continuity can't wait
April 8, 2026
Welcome back to Lumina Care's quarterly newsletter.
Each quarter, we examine a fundamental question facing care delivery across settings, with a particular emphasis on post-acute, long-term, and community-based care.
This quarter, we explore: Why do some patients make it home safely and others end up back in the hospital within days?
Transitions are clinically complex and dangerous
The answer, more often than not, comes down to what happens between settings. Not just during a hospital stay or a SNF admission, but in the handoff itself.
Care transitions are among the most clinically complex moments a patient faces.
Medications change, follow-up can be unclear, and a familiar care team disappears from view. This is complicated by the support patients have or lack outside a care facility and other social determinants of health (SDOH).
Transitions create risk that isn’t distributed evenly across the days following a discharge from hospital to SNF, or SNF to home. It concentrates in the first two days.
The Transitions Checklist
Do patients leaving our facility have a clear, documented follow-up plan they understand?
Is detailed clinical context (medications, labs, care plan changes) being transferred to specialists and providers?
Do we know which patients are highest-risk in the days immediately after discharge?
In this issue, we look at what the research says about transition risk, what coordinated care management actually changes, and what it looks like when Transitional Care Management (TCM) is running well in practice.
Study Spotlight: Transitions home for heart failure patients are a moment of critical risk
A retrospective cohort study reviewed over 60,000 patients who were hospitalized for heart failure (HF) as they were discharged to a SNF and then home over 3 years (Journal of American Medical Directors Association).
Even though 24.2% of patients were readmitted during their SNF stay, the transition home was the most dangerous moment for patients.
The hazard of readmission or death was significantly higher on days 0–2 than on days 3–30.
The first two days after going home presented the greatest risk to patients. This highlights how concentrated the risk during handoffs is for patients transitioning from a SNF stay.
Patients leaving SNFs are not stepping out of a static environment and returning home for nominal recovery. During the SNF stay, medications may be started or adjusted, labs may still be pending, and diets or treatment plans may be evolving. That means the transition home is not just a change of address. It is a transfer of clinical context, and any disruptions in continuity during transitions matter.
Transitional Care Management and coordinated care reduce readmissions
The evidence is clear: when care transitions are actively managed, outcomes improve measurably and consistently.
Within a single health system, TCM can achieve remarkable results. At Dartmouth Health in New Hampshire, a structured TCM program decreased readmissions by 58%—from 11.9% to 5% (Journal of the American Board of Family Medicine).
What made the difference wasn't any single intervention. It was the combination. The Dartmouth study found that TCM only produced meaningful outcomes when all 3 components were implemented together as a system:
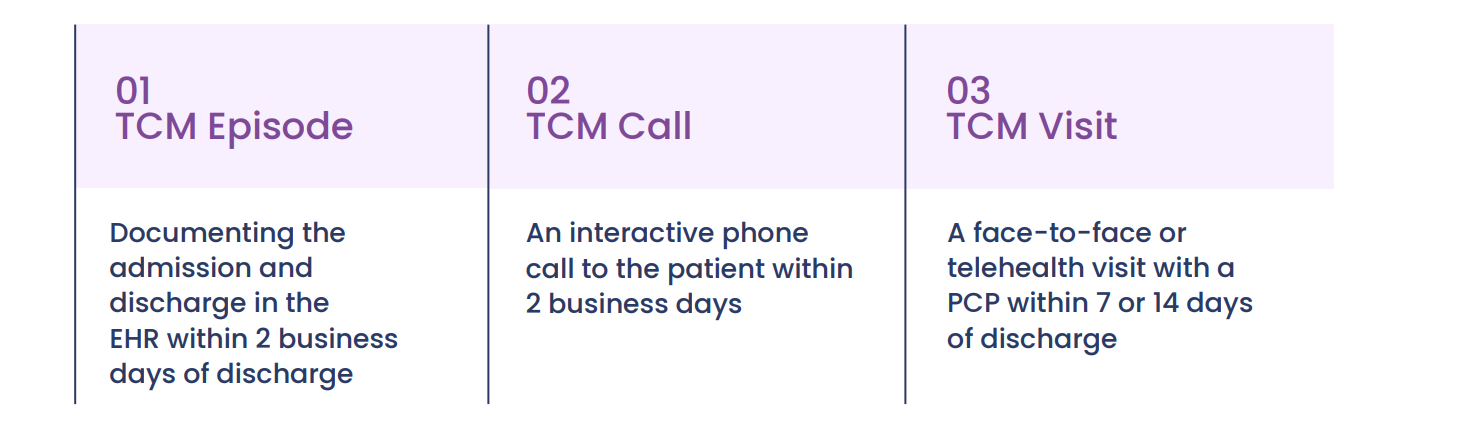
Individually, none of the 3 components moved the needle. Together, they cut readmissions by more than half.
A Health Affairs study of more than 1.6 million eligible hospital discharges reinforces the financial case: patients who received TCM reduced Medicare spending by more than $500 in the 31–60 days following discharge.
Investing in TCM builds a culture of coordination that improves outcomes across the board. The challenge is that this infrastructure remains underdeveloped across much of the care system.
Only 14.5% of eligible hospital discharges involved TCM (NORC). That means the majority of eligible patients are transitioning without structured support.
TCM in Practice: A Lumina Care Case Study
The numbers above aren't hypothetical. Here's what TCM looks like when it's running well.
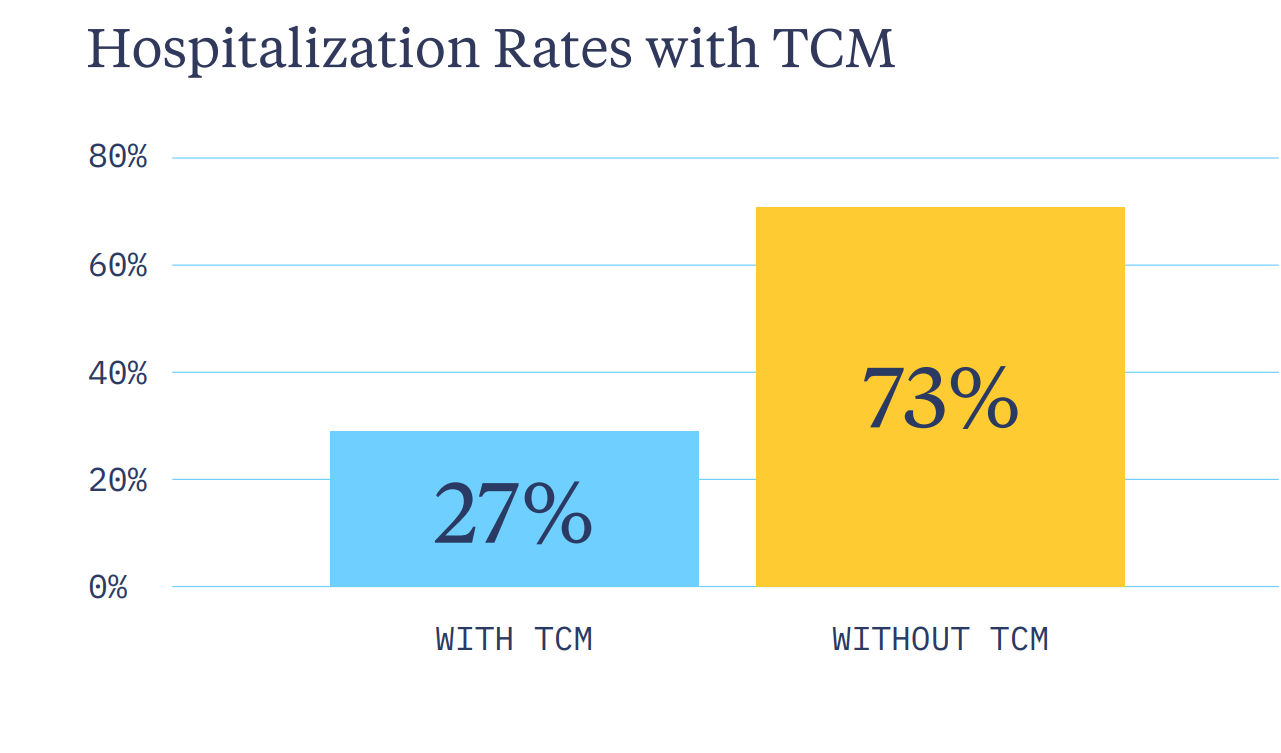
Across a multi-facility partner network, Lumina Care tracked hospitalizations month-over-month from program launch through January 2026.
In every measured month, patients with TCM had lower hospitalization rates than those without. By January, the gap was clear:
These results were driven by:
- Coordinated handoffs before discharge
- Ongoing clinical communication when complications arose
- Services ordered proactively — home health, DME, skilled nursing support, specialty prescriptions
That's coordination in practice: not reactive, but proactive.
Look Out for Lumina Care
AHCA Quality Summit
April 13-15, 2026
Baltimore Marriott Waterfront
Baltimore, MD
New Feature: Lumina360 care analysis dashboard

Better visibility changes what's possible in complex care. Lumina360 connects with PointClickCare and your EHR to track trends, flag compliance needs, and help your team act before small issues escalate.
Learn more at luminacare.com/360
Continue the Conversation
In subsequent issues, we’ll continue to explore how care breaks down or improves with continuous execution, operational trust, and identifying the truth that preventative care is a system, not a tactic.
Follow us on
LinkedIn, where we explore care delivery, quality, and consistency across care settings, systems, and specialties.



